When it comes to hemorrhagic(bleeding) stroke, there is the good news and the bad. The bad news: It is a very critical (life threatening) condition. The bleeding will build up in a contained structure (brain and skull) leading to high intracranial pressure which can suppress the overall structure of the brain leading to its lack of oxygen and demise. During my clinician days, the first rule of stroke alert is an immediate CT scan to check the brain. If bleeding ( as opposed to clogging or blocking) is present, the size of the bleed is measured ( through CT and MRI). If it is very large or it causes a midline shift, which means the pressure is shifting the position of the brain, a neurosurgical intervention is emergent.
///
[from PubMed]
Treatment of hemorrhagic stroke focuses on controlling the bleeding and reducing pressure in your brain caused by the excess fluid.
After a hemorrhagic stroke, surgery through the skull (craniotomy) might be required to remove the blood and relieve pressure on the brain if the area of bleeding is large enough. Surgery may also be used to repair blood vessel problems associated with hemorrhagic strokes. Your physician may recommend one of these procedures if an aneurysm, arteriovenous malformation (AVM) or other type of blood vessel problem caused your hemorrhagic stroke:
- Surgical clipping. A surgeon places a tiny clamp at the base of the aneurysm, to stop blood flow to it. This clamp can keep the aneurysm from bursting, or it can keep an aneurysm that has recently hemorrhaged from bleeding again.
- Surgical AVM removal. Surgeons may remove a smaller AVM if it’s located in an accessible area of your brain. This eliminates the risk of rupture and lowers the risk of hemorrhagic stroke. However, it’s not always possible to remove an AVM if:
- It is located deep within the brain.
- It is simply too large.
- Its removal would cause too much of an impact on brain function.
[from PubMed]
///
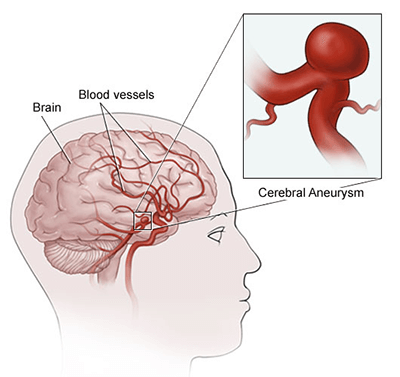
If an aneurysm is likely to rupture, a variety of surgical procedures can divert blood flow away from the aneurysm and repair the affected blood vessel, including microsurgical clipping, artery bypass and occlusion, flow diversion with stents and endovascular coiling.
The most common symptom of brain aneurysm is a headache so unexpected, worse than a migraine. I had patients describing it as the most painful headache they have experienced.
Now the good news: Sometimes the bleed is so small that the Neurologist will just let it be reabsorbed until it eventually disappears. This is the best outcome scenario. The other good news: bleeding stroke though critical in the acute phase usually shows a rather better outcome in recovery with less disability and shorter recovery period as opposed to infarction.
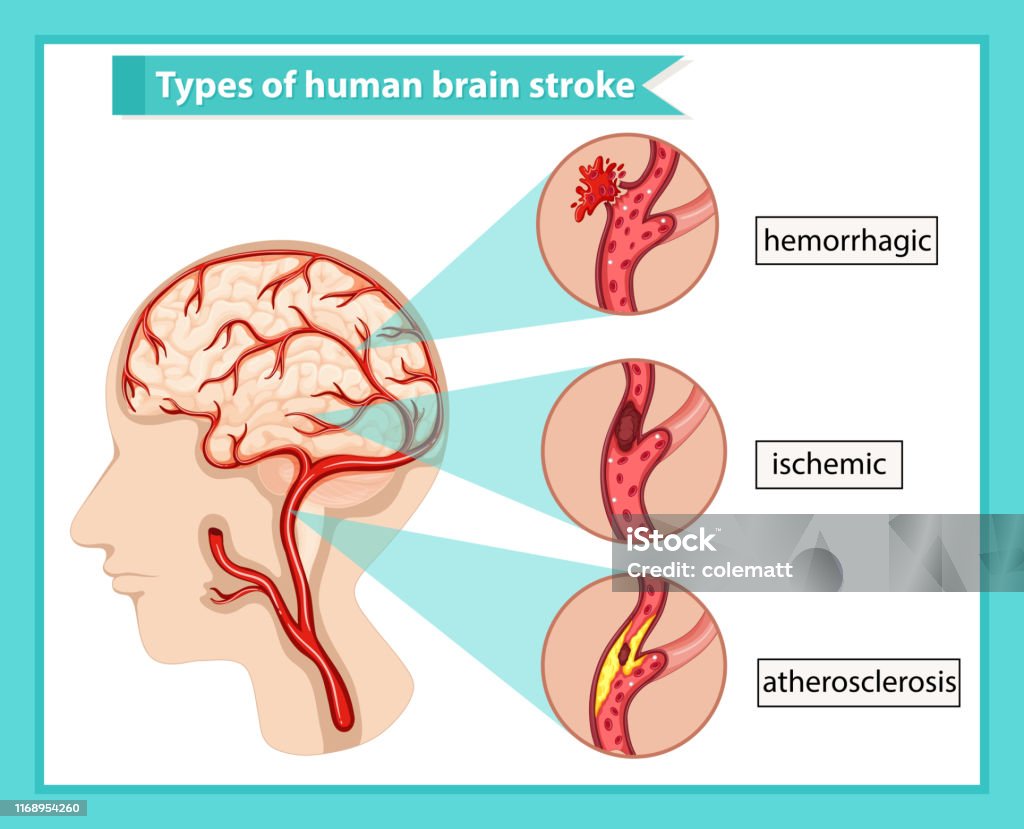
***How about a clogged (infarction) stroke? There is a surgical hope for people with clogged (infarct) strokes as well. Besides the tPA during the first 3 hours that can potentially reverse it; there is also a neurological procedure called thrombectomy.
///
Thrombectomy is a medical procedure used to treat some cases of ischaemic stroke. This type of stroke is caused by a blood clot blocking blood flow to part of the brain and accounts for around 85% of strokes.
Thrombectomy is a treatment to remove the blood clot. It should be carried out within the first six hours of a stroke starting to be most effective. If you experience stroke symptoms, it’s important to get to the hospital as quickly as possible for treatment and to see if you’re eligible for the procedure.
///
In conclusion, there are different causes for stroke and they can be minimized by lifestyle changes. Let me repeat the keyword ‘minimized’ here, not a complete immunity. Anybody, including myself can have a stroke for any possible unknown cause. Anybody can have afib without knowing it, can have high blood pressure without knowing it, can have genetically weak blood vessels that can balloon and rupture without knowing it, can develop a blood clot in the leg without knowing it.
I used to work in the acute phase of stroke during my clinician days. I start moving the patient when appropriate as determined by the Stroke Team (yes, advanced hospitals certified as Comprehensive Stroke Centers have Stoke Teams). My role was the least glamorous. Under close monitoring, I get you up, transfer you to a chair, gradually walk you until ready for home or rehab or an SNF. There are lots of cases whose strokes get reversed and they go home. There are those who might need a short term rehab to facilitate going home. There are those who may need long term care and they are transferred to Nursing Homes. And then, there are cases called ‘stroke in evolution’ that I pay very close attention to. These are strokes that are still in progress and it is a must to monitor things like increased confusion, increased drowsiness or seizures. And immediately alert the Stroke Team again if needed.
But I am not here to blog about how I manage patients with stroke. There are many Doctors and Therapists and Nurses who deal with the medical and recovery aspects of Stroke. Each of these members have their own specialties and sub-specialties. I am limiting myself to basic information that may help a layman in understanding what stroke is and how to manage one’s lifestyle to minimize the risk of having it.
Evidence-based lifestyle changes can help. The first rule is a regular check up, like a car, to see abnormalities in the system whether it is in the blood pressure, blood sugar, bad cholesterol and well, lets face it, body weight. Obesity is not a good protection from stroke. If blood work finds abnormalities in any of the tests, by all means take the prescribed medications.
The next rule is lifestyle. We may not be able to control the medical factors that predisposes somebody to stroke - old age, heart diseases, blood vessel diseases, diabetes, kidney diseases - but there are factors we can control.
Stop smoking, avoid abusing alcohol, avoid eating bad food that worsens blood pressure (high salt), or diabetes (high sugar and carbohydrates).
Work on proper nutrition and diet, exercise, reduce stress (that can increase BP, sugar) and when it comes to stress, it can be physical and mental or both.
Physical stress refers to any activity that is inappropriate for one’s age, An example is assuming you can still do (in your 50s) what you used to do in your twenties whether it is sports or gym work-out or running marathons. It is more prudent to scale the exercise down as you get older, (not to avoid exercising completely) but scaling it down. Physical stress can also be environmental. Too much air pollution, super hot weather (heat wave), overworking no matter how much you love your work, chasing after cars and trains and any form of transport because you are late or in a hurry, climbing multiple stairs when the elevator is not working, deciding to play golf with old buddies out on a whim and you play the whole day ( I had a stroke patient who did just that), trying to show off with the ladies that you are super macho by lifting some heavy loads too much for your strength. There are lots of things you need to reconsider when you turn over 50 or 60 to prevent stroke.
And then, there is the mental stress. Avoid toxic relationships or engagements whether it is with family (spouse or children or relatives) even with your ex-friends and neighbors. If someone triggers anxiety or anger or fear inside you, avoid that person. That holds true with situations. If you are stressed out because you are forced to do something you don’t want to do - an introvert who is thrusted to a noisy party or an extrovert being imprisoned in a lonely isolation - please be nice to yourself and leave. Working relationships that make you squirm or pause for fight or flight reaction is not healthy either Sometimes, social media can be toxic. If you are dealing with toxic FB friends who have all the time in the world to judge or bully or harass you, learn to turn off your screen or phone to ignore them.
There is a time to plant and a time to harvest, a time to work and a time to rest. Being over 50 is probably the peak of one’s life. This is the age you’ve earned what you worked hard for. You are respected for your experience, trusted by most for being reliable and your confidence is more secure because you’ve been there and done that.
The 60s however is the laurel of your life. There are no more heavy responsibilities if you have played your cards right during your working years. This is the decade of winding down. Mortgage has been paid, the kids are no longer dependent on you, gone are the challenges and struggles to support your family and you are done trying to prove your worth. You are sure of yourself without a care about what others think about you. You do what pleases you and damn the bitter enemies LOL. You probably have set the bar lower when it comes to finding love and social connections. Me? I personally don’t even care if I were treated non-existent by the world around me. I don’t mind not getting second looks. This is the age you can enjoy life fully provided you are prepared for it properly. You may have a steady income, like social security, that you worked hard for. Some may even have over-saved and accumulated wealth through proper investments, so now they have more money than what they need. They travel, go to expensive restaurants, watch movies, hang out with old friends, spend time in bingo or cruise ships, they deserve it.
And then there are people like me who are closet introverts. I will talk more about introverts when I review the book ‘Quiet’ by Susan ___ in my next book review.